Radiofrequency Ablation of Spinal Osteoid Osteomas
Osteold osteomas are not uncommon in the spine and often present diagnostic difficulties. However, once an osteoid osteoma has been diagnosed in the spine, it becomes necessary to decide among the various treatment options.
As in the appendicular skeleton, radiofrequency ablation (RFA) is a definite option for treating spinal osteoid osteomas, wherein we can introduce an electrode into the lesion and burn it.
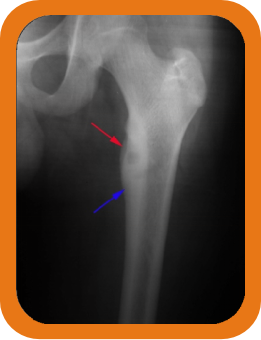
The use of RFA however depends a lot on the location of the lesion, since there is always a potential risk of damaging the cord, thecal sac or nerve roots. If it is far away from these structures, then the procedure is quite straightforward (Fig. 1). Even if it is near the nerve root, if there is enough cortical bone between the lesion and the nerves, then too, there is no problem (Fig. 2).
However when the lesion does not have adequate cortical bone between it and the nerve and thecal sac, additional measures have to be taken to ensure that there will be no damage to the nerves (Fig. 3). These include, ensuring that the electrode points straight towards the thecal sac, using epidural or foraminal air (air is a poor conductor of heat) or dripping cold distilled water into the epidural or foraminal space.
If RFA can be done safely, as in all the three cases shown, the results are quite rewarding. with virtually instantaneous relief of pain.
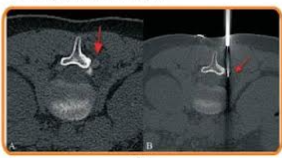
Fig 1. AB Prone ast CT scan (A) shows an ostama jarrow) adjacent to the 12 pedicle on the undersurface of the transiran process. This is far away from the thecal sac and nerve mut, The prone asiar C scan (2) shows the position of the electrode (ar) and the son was safely and eanly bed with comple
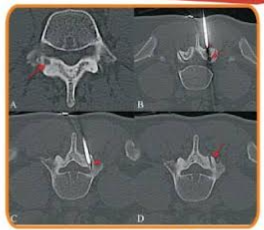
Fig. 2(4-0) Super axial CT scan (A) shows an ostrostom (arrow) involving the junction of the right pedicle and lamina of Prone axial CT scans (BC) show that the lesion (arrow) Covered by the overly facet joint and hence then enough bone around it to prevent heating of the adjacent structures. The initial (arrowhead in and final arrowhead in C position of the needle tip and electrode are shown, along with the ha tract (pw in allowing successful procedure.
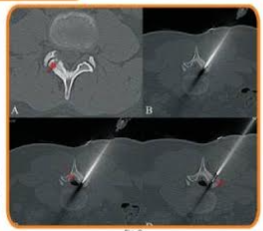
Fig 3/ADSCT scan (shows an oste uteom (now) oving the right 3 in with very this bone separating the fision from the spinal canal The need was directed right towards the spinal canal and thecal soc arrow in since heating beyond the tus of the needles for less than around Epure air (arrow in C) was introduced to seperate the theal sac further from the laminas. The fil position of the electrode prior to the ablatin is shown (arrow in 0 Post abiation, the patient was pain free within 48 hours.