Radiofrequency Ablation (RFA) of Lung Tumors
Radiofrequency Ablation (RFA) of Lung Tumors
Bronchogenic carcinomas are traditionally treated with surgery, and / or with radiotherapy / chemotherapy, depending on the stage of the lesion and the physical condition of the patient.
Radiofrequency ablation (RFA) is a relatively new technique that is used to treat tumors in different parts of the body using the principle of thermal ablation. The initial results in hepatomas and liver metastases were extremely encouraging, leading to an expansion of the indications of RFA in the lung, kidney, adrenal glands, retroperitoneum, thyroid and breast.
Procedure
- The study is performed under deep sedation and anesthetist consent is taken.
- The coagulation profile has to be normal.
- The exact route is planned so that the electrode can be introduced along the long axis of the tumor, upto the centre with minimal damage to the adjacent structures
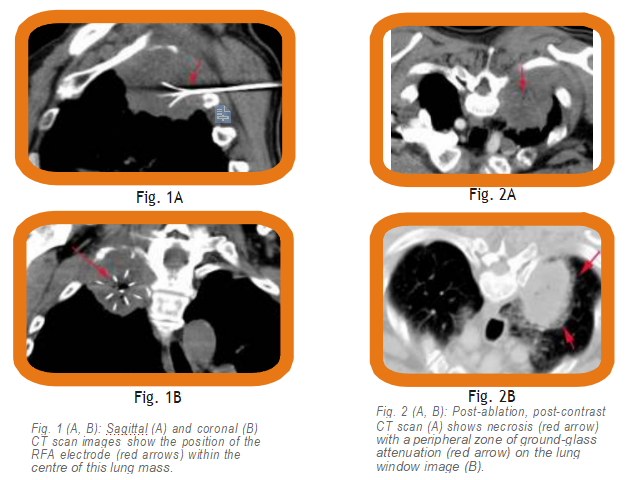
- After the electrode is introduced (Fig. 1), the tumor is ablated to 90 deg for 6 minutes for every volume cm of ablation starting from 3cm. For e.g. a six cm tumor may take upto 4 x 6 minutes for ablation
- After the ablation is done, a check CT is performed to look for necrosis and the zone of ground-glass around the lesion, which usually suggest technical success (Fig. 2).
The procedure is performed on an OPD basis and unless there is complication (hemothorax, pneumothorax), the patient is allowed to leave as soon as the effect of the anesthetic wears off.
Indications
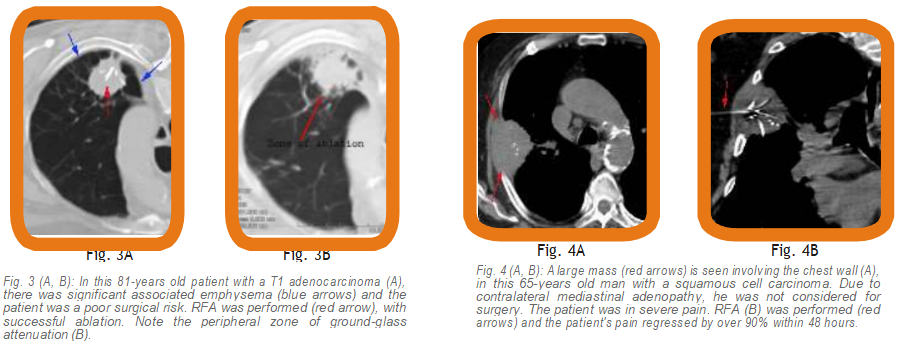
- Thelesion is ideal for surgical excision, but the patient is not a candidate for surgery, due to co-morbid conditions (Fig. 3).
- For pain relief, when the mass involves the chest wall and ribs (Fig. 4).
- Metastases,when surgery is difficult.
Contra-indications
- No direct route available
- Anesthetist refuses to give sedation
- Abnormal coagulation profile
All papers in literature have shown that if the lesion is successfully ablated, there is no progression of the primary disease and there is increased survival. In those patients with severe pain, due to rib or chest wall involvement, RFA produces significant pain relief. Death is usually due to unrelated factors or metastatic spread.